

Stay Present With the Patient. SPRY Takes the Note From Visit to Billing.
SPRY listens during the visit, generates the SOAP note in your clinical voice, and moves it toward billing. So you can focus on care, not screens.
Book a DemoTrusted by 500+ Rehab Therapy Clinics

Documentation Burden Affects Care Quality,
Compliance, and Cash Flow.
Less time with the patient
Therapists split attention between care and charting during the visit, or carry documentation into breaks and after-hours work.
Inconsistent, incomplete notes
Manual documentation makes it harder to maintain complete, compliant, audit-ready records across clinicians and locations.
Slower billing cycles
When notes, co-signs, and required details are delayed, claims cannot move forward cleanly and billing teams inherit the rework.
One DocumentationWorkflow,
From Visit to Claim
Patient context, AI Scribe, templates, co-signs, compliance checks, and billing readiness stay connected from the moment care begins.
How SET PT Made Documentation Easier Without
Compromising One-on-One Care
AI-assisted SOAP notes helped SET PT clinicians stay more present during sessions, complete notes on time, and improve clinical continuity across visits.
"Being able to actually record the session—or parts of the session—has been a game changer for us."
- Stacy Hund, DPT
THERAPY
From After-Hours Charting to Billing-Ready Notes
SPRY changes what documentation feels like for therapists — and what it unlocks for the clinic.
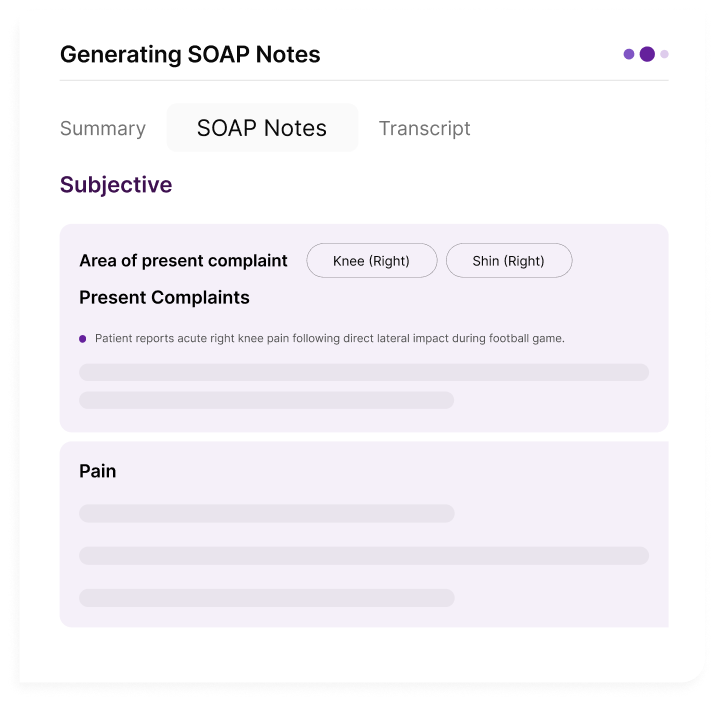
Notes That Speak the Language of Rehab
See how SPRY generates specialty-specific SOAP notes shaped by the measures, goals, and clinical details that matter in each workflow.
Pain 3/10 at rest, 6/10 with overhead reach. Sleep tolerance improving.
Shoulder flexion 110°, abduction 95°, ER 30°. Strength remains limited with overhead movement.
Progressing toward post-operative ROM goals. Functional elevation remains restricted.
Advance strengthening per protocol. Continue reaching tasks and home exercise program.
Reports improved confidence with running. Mild hesitation during cutting and landing drills.
Single-leg squat control improving. Hop symmetry remains reduced on the involved side
Strength and dynamic stability are progressing, with residual deficits during higher-demand tasks.
Advance agility, deceleration, and sport-specific return-to-play drills.
Difficulty with dressing and meal prep. Pain increases with wrist extension and sustained grip.
Wrist extension 25°, flexion 40°. Grip strength remains reduced on the involved side.
Limited ROM and grip strength continue to affect ADL independence.
Continue therapeutic exercise, fine motor work, and task-based retraining for daily activities.
Reports greater confidence walking at home. No falls since last visit.
Gait speed and transfer performance improving. Left foot clearance remains reduced during swing phase.
Functional mobility is improving, with ongoing weakness affecting gait efficiency.
Progress uneven-surface training, dual-task walking, and lower-extremity motor control work.
Continued urgency and stress leakage with coughing and exercise. Symptoms gradually improving.
Pelvic floor strength 3/5 with delayed deep core activation and reduced endurance.
Coordination and activation are improving, though weakness continues to affect symptom control.
Advance pelvic floor coordination, breathing mechanics, and graded return-to-exercise progression.
Neck stiffness reduced since last visit. Fewer headaches and better tolerance for desk work.
Cervical rotation and extension improving. Residual tenderness noted through upper trapezius and paraspinals.
Responding well to care with improving mobility and reduced symptom irritability.
Advance strengthening per protocol. Continue reaching tasks and home exercise program.
COMPLETED
Caregiver reports the child is pulling to stand more often at home but still avoids cruising along furniture.
Tolerated supported standing for 45 seconds. Required moderate facilitation for lateral weight shifting and sit-to-stand transitions.
Improving lower-extremity engagement and standing tolerance. Motor planning and confidence with lateral movement remain limited.
Continue play-based strengthening, supported cruising activities, caregiver education, and home practice routine.
COMPLETED
Parent reports increased use of single words at home, especially during meals and play routines.
Produced 12 spontaneous single-word utterances during structured play. Imitated two-word phrases with moderate verbal and visual cues.
Expressive vocabulary and imitation are improving. Continued support needed for phrase expansion and functional communication.
Continue play-based language intervention, parent coaching, and two-word phrase modeling for daily routines.
COMPLETED
Patient reports feeling steadier when rising from a chair but still avoids walking outside alone.
Sit-to-stand improved from 5 reps to 8 reps in 30 seconds. Requires supervision with obstacle negotiation.
Lower-extremity strength and transfer confidence are improving. Dynamic balance remains a safety concern.
Continue balance training, transfer practice, gait progression, and home safety education.
COMPLETED
Patient reports mild stiffness in the morning and improved tolerance with light daily tasks.
Digit flexion improving with mild edema noted. Grip strength remains limited compared to uninvolved side.
Progressing appropriately with ROM and functional use. Continued limitations with swelling control and grip strength.
Continue protected ROM, edema management, graded strengthening, and home exercise program per protocol.
COMPLETED
Patient reports dizziness has reduced with daily activity but symptoms still occur when turning quickly.
Gaze stabilization tolerated for 45 seconds with mild symptom increase. Balance testing shows increased sway on uneven surface.
Vestibular tolerance is improving. Dynamic balance and quick head movement remain symptom-provoking.
Continue gaze stabilization, habituation exercises, balance progression, and fall-prevention education.
Everything Needed to
Complete the Note,Built In
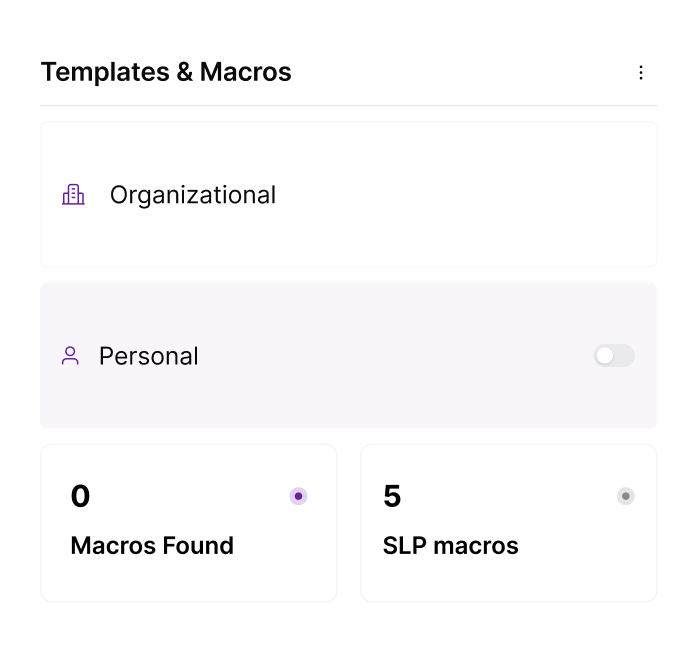
Custom Templates and Macros
Supports provider-specific shortcuts, specialty templates.
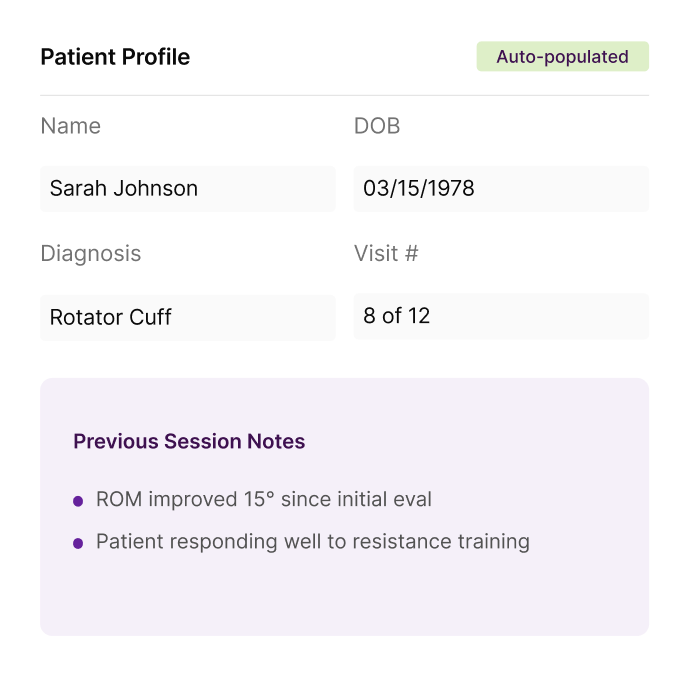
Carry-Forward Context
Brings forward prior notes, goals, objective measures, visit history, and plan details.
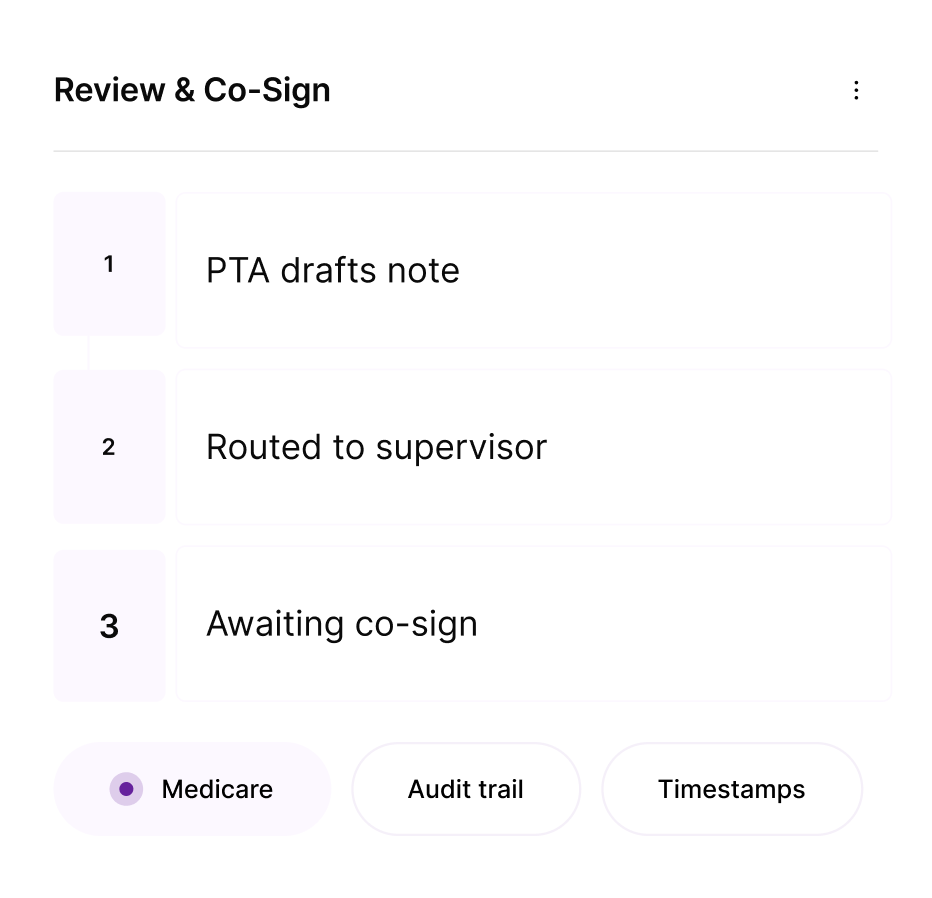
Co-Sign and Supervision
Routes PTA notes to supervising PTs with review status, approvals, timestamps.
Compliance Checks
Flags missing fields, signatures, care plan gaps, auth context, and payer-required documentation.
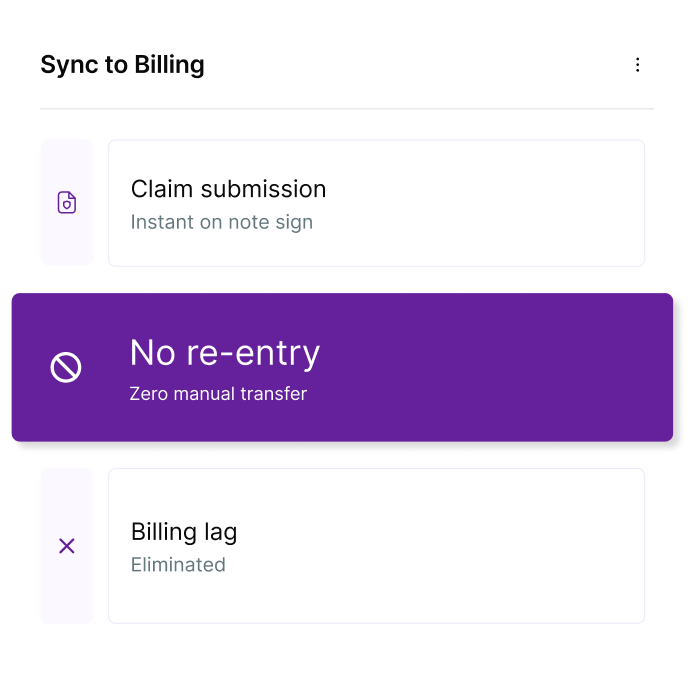
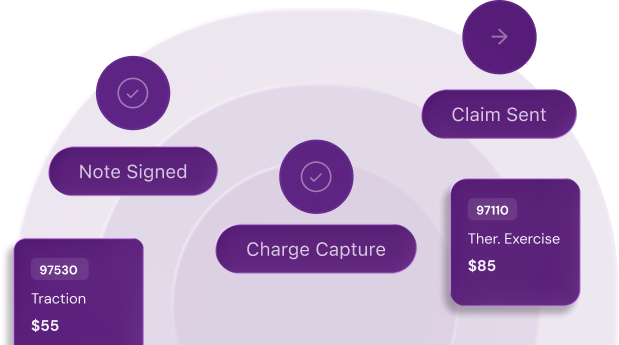
Billing Connection
Moves signed notes toward charge capture and claim submission without duplicate entry.
Documentation Reporting
Tracks incomplete notes, pending co-signs, provider bottlenecks, and documentation status.
Less Time Charting.
More Clinical Capacity Back.
SPRY does more than shorten the note. It gives therapists time back during and after the visit, helps clinics close documentation faster, and returns meaningful clinical capacity across the team.
5 therapists × 54 minutes/day × 5 days/week × 48 weeks
Time that can go back into patient care, same-day documentation, and a clinic that runs with less after-hours charting.
See the impact for your clinic
Book a Demo →
Hear How Therapists Stay Present, Finish Notes Faster, and Document With Confidence
Got questions? We’ve got answers.
Need more help? Reach out to us.